When Something Feels “Off”: Understanding Laryngeal Cleft & Submucous Cleft March 2026
Sometimes a child struggles with feeding, reflux, coughing, or speech — and everyone keeps trying therapies, medications, and positioning… but something still doesn’t quite add up.
This month, we’re discussing two structural differences that are often overlooked:
Laryngeal Cleft
Submucous Cleft Palate
These are rare — but important to recognize.
What is a Laryngeal Cleft?
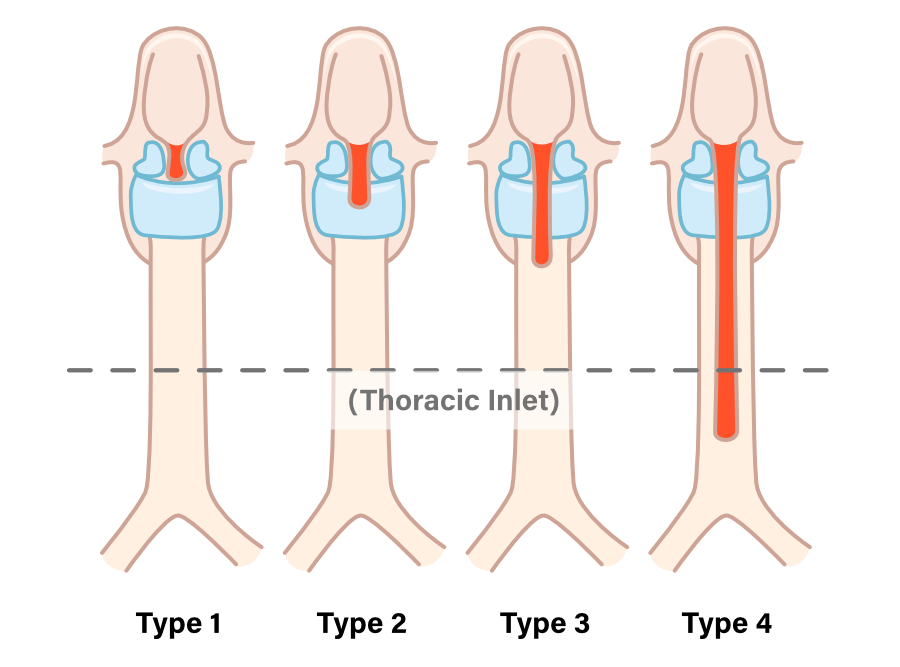

A laryngeal cleft is an abnormal opening between the airway (larynx) and the esophagus.
Normally, these two tubes are completely separated:
One for breathing
One for swallowing
In a laryngeal cleft, they are partially connected, allowing food and liquid to slip toward the airway.
Common Signs & Symptoms:
Chronic coughing with feeds
Recurrent pneumonia
Frequent respiratory infections
Noisy breathing
Stridor
Cyanosis during feeding
Poor weight gain / Failure to Thrive
“Reflux” that doesn’t improve with medication
Wet or gurgly voice after eating
Some children have NO obvious coughing
Important: Not all children cough. Some silently aspirate.
How Is It Diagnosed?
Direct laryngoscopy under anesthesia (gold standard)
Modified Barium Swallow (may show aspiration)
FEES (Fiberoptic Endoscopic Evaluation of Swallowing)
A swallow study alone does NOT rule it out.
What is a Submucous Cleft Palate?
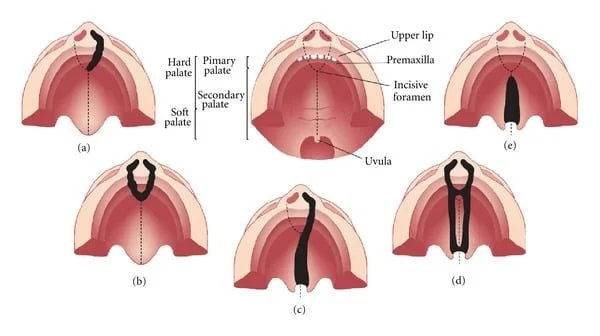

A submucous cleft palate is a hidden cleft.
The outer lining of the palate looks intact — but the muscle underneath did not fully fuse.
It can be easy to miss.
Classic Signs:
Bifid (split) uvula
Thin blue line down midline of palate (zona pellucida)
Notch at back of hard palate
Hypernasal speech
Air escape through nose when speaking
Nasal regurgitation of liquids
Feeding fatigue in infancy
Sometimes children compensate early — and it’s not discovered until speech becomes more demanding.
How Are These Two Different?

When Should Families Ask Questions?
If you notice:
Persistent feeding struggles despite therapy
“Reflux” not responding to medication
Recurrent pneumonias
Hypernasal speech
Food or liquid coming from the nose
Thin hair, poor growth, unexplained fatigue
Development that doesn’t match the full picture
It is okay to ask your physician:
“Could there be a structural reason for this?”
Sometimes the missing piece is anatomical — not behavioral.
Therapy While Awaiting Evaluation
While further testing is being considered:
Consider thicker liquids if aspiration suspected (guided by SLP)
Avoid forcing feeding
Monitor respiratory patterns
Support safe oral exploration
Encourage humming to assess velopharyngeal closure
Gentle airflow tasks (watch for nasal escape)
Crying alone does NOT fully evaluate palate function — structured speech tasks are needed.
A Gentle Reminder
Not every child with reflux has a cleft.
Not every child with speech differences has structural concerns.
But when something feels persistently unresolved — digging deeper can change everything.
At Star Center Foundation, we believe in:
Bridging care with compassion
Looking beyond surface symptoms
Supporting families through clarity, not confusion.
If you would like an evaluation or guidance:
Star Center Foundation
835 Sharon Dr, Suite 280
Westlake, OH 44145
216-320-2456
starcenterfoundation.org